Pilot Study on Predictors of Vaccine Hesitancy among Muslim-Americans: The Roles of Trust, Religiosity, and Political Beliefs
Marina Ali,William Sorensen,Cheryl Cooper
1 Texas Health HEB/Denton Internal Medicine Residency, Bedford, Texas, USA
2 University of Texas in Tyler, Tyler, Texas, USA
3University of Texas in Tyler, Tyler, Texas, USA
Email: marinali2@texashealth.org, wsorensen@uttyler.edu, ccooper@uttyler.edu
Background: Vaccine hesitancy hinders the management of preventable illnesses. Currently, there are gaps in public health research on vaccine hesitancy among Muslim-Americans. There are few studies that examine Muslim-Americans in multi-faith countries, like the U.S. and Canada.
Objective: We aimed to understand the extent of vaccine hesitancy among Muslim-Americans, as well as what factors contributed to their health care decision making for vaccines.
Method: Participants were recruited through Facebook group posts. Seventy-three participants completed the online Qualtrics survey. Sixty-five participants met the inclusion criteria of living in the United States for at least five years, be eighteen years of age and identify as Muslim. Participants’ responses were collapsed into the following belief scores to quantify subjective opinions from the survey: political leaning, religiosity, trust in public institutions, and vaccine hesitancy.
Results: 71.4% were female, with an average age of 32 years. 80.6% were Asian, 9.7% were white or Caucasian, 3.2% were Middle Eastern, 3.2% were mixed race, and 1.6% were Black or African American. 51.6% attained a graduate or doctoral degree. 79.0% identified as Sunni, 9.7% were Shia, 6.5% were Sufi, and 4.8% did not associate with a sect. 96.8% received at least one dose of the COVID-19 vaccine. Participants who were older in age, had attained higher levels of education, employed, unmarried, and identified with the Sunni sect were less vaccine hesitant. Most participants (36.5%) were more likely to accept a vaccine if it had no reported safety issues. Participants were more likely to be hesitant about vaccines with safety concerns or poor efficacy.
Conclusions: Results both align with and contradict previous studies conducted in Muslim majority and multi-faith countries. This study found an association between Islamic sect and attitudes towards vaccines. While this is a unique finding, it is exploratory. Follow up studies are necessary to gauge a larger, more diverse population of MuslimAmericans. Based on this study’s findings, healthcare professionals can better promote vaccines by alleviating their patient’s trust in public institutions. Clinicians must understand their Muslim patients’ fears about vaccination and address misconceptions. Public health institutions must engage in culturally relevant community-level advocacy and education. Mistrust by Muslim-Americans stems from a history of systemic discrimination, Islamophobia, and socioeconomic barriers to adequate healthcare. Thus, solutions must emphasize improving healthcare access for Muslim-Americans and helping them feel reassured about the healthcare system at large. We suggest incorporating translation services for better communication. We recommend that clinicians emphasize positive attributes of vaccines that align with accepted beliefs within Islam, such as protecting the community.
Keyword: vaccine hesitancy vaccines Muslim health Muslim-American
Pilot Study on Predictors of Vaccine Hesitancy among Muslim-Americans: The Roles of Trust, Religiosity, and Political Beliefs
Marina Ali,William Sorensen,Cheryl Cooper
1 Texas Health HEB/Denton Internal Medicine Residency, Bedford, Texas, USA
2 University of Texas in Tyler, Tyler, Texas, USA
3University of Texas in Tyler, Tyler, Texas, USA
Email: marinali2@texashealth.org, wsorensen@uttyler.edu, ccooper@uttyler.edu
INTRODUCTION
Vaccine hesitancy refers to delaying vaccination, questioning their efficacy or expressing doubt in their safety [1]. Vaccine refusal is the complete rejection of vaccines [1]. Anti-vaccination sentiments are known to increase the proliferation and death rates of preventable illnesses, while also putting immunocompromised and nonvaccinated populations at risk. There have been studies, like those by Hossain et al. [2] and Sallam et al. in 2021 [3], that were conducted in Muslim majority countries. However, there is still no consensus on Muslim communities as a whole group in multi-faith societies, like the United States. Such studies focus on MuslimAmerican subgroups. For example, Hearld & Budhwani [4] studied Muslim-American women. Due to this research gap, our study aimed to understand MuslimAmerican vaccination trends. We hypothesized that Muslim-Americans had similar vaccination trends and factors for vaccine hesitancy as the larger American populace.
Vaccine Hesitancy Trends in America
There are numerous trends in vaccine hesitancy and denial among Americans. Parents who believed strongly in vaccine adverse effects, distrusted institutions, had a feeling of helplessness, questioned vaccine efficacy, or desired bodily autonomy, were more likely to express vaccine hesitancy or outright deny them for their children [5]. University students were more likely to accept a vaccine if they perceived that a vaccine-preventable disease caused immense physical suffering or had a family member who contracted the illness in the past [6]. Americans who distrusted public institutions, like the CDC, were older in age, childless and less educated, and were more likely to be vaccine hesitant [7]. In 2020, 6% of parents were hesitant against routine childhood vaccines and 25.8% were hesitant against flu vaccines [8]. Low efficacy and the potential risk of side effects were cited as the most important factors for avoiding vaccines [8]. Parents of lower socioeconomic status, Hispanic heritage and fewer years of education were more likely to be hesitant [8].
Vaccine Hesitancy Among Muslims
Most studies on vaccine hesitancy among Muslims were conducted in Muslim majority countries. For example,96.1% [9] and 80% [10] of Saudi parents supported vaccination in 2021 and 2019, respectively. 92% [11] and 88.4% [12] of Malaysian parents supported vaccination in 2020 and 2017, respectively. Pakistani parents in Taliban controlled areas were 23% to 39% less likely to vaccinate their children compared to parents in non-Taliban controlled areas [13]. 68.4% of Nigerian mothers accepted vaccines [14]. Some studies combined data from multiple countries. For example, Owoaje et al. [15], who analyzed vaccine hesitancy trends in Afghanistan and Nigeria. 18 Arab nations aggregated vaccine acceptance rates of 29.4% and 30.9% in 2021 for COVID-19 and influenza immunizations, respectively [3]. Other studies contained samples from countries with Muslim minorities, such as 61% of the children in a Muslim-dominated area of Ethiopia received regular vaccinations [16].
Knowledge Gaps
There are no consistent vaccine hesitancy trends in Muslim communities living in multi-faith countries, like the United States and United Kingdom [17]. Therefore, most information about western Muslims is found in secondary sources. For example, in 2017, there was a highly publicized outbreak of measles in the SomalianMuslim diaspora in Minnesota. Public health officials cited the increasing anti-vaccine sentiments within the community as the primary cause of the outbreak [18]. Vaccine hesitancy studies in multi-faith countries typically cast a wide net. For example, 65% of Irish and 69% of British people accepted vaccines in 2021 [19]. Unfortunately, religion was not studied in this sample, so it’s unclear if there were any religious associations with vaccine sentiments.
Themes
In past studies, there were several factors that influenced Muslim parents’ willingness to vaccinate their children, such as religious prohibitions [20], parental experience [3], level of trust within public institutions [21], and political affiliations [19]. For example, some Malaysian parents were concerned about vaccine ingredients, considering how certain vaccines utilize pork byproducts during production and consuming pork products is forbidden in the Islamic tradition [22].
Methods
Study Design
We designed a cross-sectional, quantitative study. Participants completed an online survey on the Qualtrics platform; they were convenience and snowball sampled. Data collection began in May of 2022 and was completed 2 months later in July. Because the study utilized an online survey, the authors utilized the CHERRIES framework [23]. A completed CHERRIES checklist can be found in Appendix 1.
Questionnaire Tool
Appendix 2 contains the full questionnaire. The survey was divided into 4 sections: demographics, religion, political beliefs, health beliefs. The following belief scores were created to quantify participants’ responses: religiosity, vaccine hesitancy, trust in healthcare institutions, and political ideology. Belief scores were quantified by assigned questions, as listed in (Table 1). Each question was scored using a Likert scale that was associated with its answers. Health belief scores were dependent variables. Generally, the higher the score, the stronger the belief. For example, a score of 5 for religiosity meant that the participant did not identify as a religious Muslim, whereas 25, which is the highest possible composite religiosity score, reflected an intense devotion.
The only exception to this rule was the political beliefs composite score, which analyzed the participant’s political stance on a scale from extremely liberal to extremely conservative. For example, participants with a score of 30, the highest possible, identified as having very conservative political and social beliefs. Not all participants could answer the question that is denoted with a superscript (a ). It inquired about children, so childfree participants were scored 0 for this question. The questions that surveyed political beliefs were split into the political beliefs score and trust in public institutions score.
|
Score Name |
Min |
Max |
# Q’s |
Question Number |
|
Religiosity |
||||
|
6 |
30 |
6 |
13, 14, 15, 16, 17, 18 |
|
|
Vaccine Hesitancy |
||||
|
7 |
40 |
8 |
32, 33, 35, 36, 37, 38, 39a, 40 |
|
|
Trust in Public Institutions |
||||
|
6 |
30 |
6 |
25, 26, 27, 28, 30, 31 |
|
|
Political Beliefs |
||||
|
6 |
30 |
6 |
19, 20, 21, 22, 23, 24 |
|
Table 1. Description of composite scores in belief category
Participant Selection
A target sample size of 43 was determined from the following parameters:
• Study Group Design: One study group vs. population
• Primary endpoint: dichotomous
• Anticipated incidence: 70% known population, 50% study group
• Alpha (α): 0.05 • Power: 0.80 (Beta (β) = 0.20)
• Power: 0.80 (Beta (β) = 0.20)
Participants were required to be at least 18 years of age, identify as a Muslim, and live at least 5 years in the U.S. at the time of completing the survey. Since there are immigrants to the United States who are Muslim, it was necessary to set a limit on what this study defines as “American.” Immigrants need a few years to acclimate and identify as a member of their new country, so it was necessary to have a set minimum amount of time to establish how well someone identifies with their residence. The inclusion criterion of 5 years was selected since the naturalization process requires that all eligible applicants for citizenship live in the country for at least 5 years [41]. Participants in the exclusion criteria did not meet all the requirements for the inclusion criteria.
The participants were recruited through 10 Muslimoriented Facebook groups. Appendix 3 is the recruitment message that was posted in the Facebook groups and Appendix 4 lists the Facebook groups that received the recruitment message. Interested individuals accessed the survey using the link provided in the recruitment message. In the recruitment message, participants were encouraged to further spread information about the study to other individuals in their social circles who met the inclusion criteria. The recruitment message was posted on the same date in May 2022, after which survey responses were collected in Qualtrics. The survey was closed in July 2022. Selection of the Facebook groups was more deliberate, because targeted recruitment could ensure a higher chance of acquiring survey responses from the inclusion criteria. Thus, groups with larger memberships and more page activity were chosen over those that did not have these qualities.
Analysis
All data analysis was completed on the IBM SPSS Statistics 28 software. First, descriptive statistics were obtained for the following demographic factors: age, gender, race, highest level of education completed, employment status, total combined household income before taxes, marital status, number of children under the age of 18, Islamic sect, political views, source of healthcare information, and factors for vaccine hesitancy. Normalcy was scrutinized. When a demographic variable was skewed, it was transformed into a normal distribution. The four belief scores were calculated for each participant. The belief scores and the COVID-19 vaccination status were analyzed using T-tests and linear regression testing to determine if there are associations with the demographic variables. Additionally, correlation was conducted with continuous output variables. Finally, multiple regression analyses were conducted using the bivariate significant values for each score. The unadjusted model was created using the “Enter” preset while the adjusted model utilized the “Backwards” preset.
Ethical Considerations
Written informed consent for involvement in the study and publication of this paper was obtained from all subjects. The informed consent statement is in Appendix 5. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of Texas in Tyler (IRB #2022-030 on May 12, 2022). Participants volunteered to be in the study; thus, they were not compensated. All study data was collected anonymously.
Results
In April of 2022, a pilot study was conducted with five individuals. After IRB approval, the website link to the survey was disseminated online to Facebook groups. Data collection began in May of 2022 and was completed two months later. 73 responses were received. 65 met the required inclusion criteria. Since 43 participants were sought, the extra responses meeting the inclusion criteria increased this requirement by 51% (65/43).
Belief Score Distributions
The distribution of the vaccine hesitancy scores is shown in Figure 1, showing a pronounced negative skew. Table 2 lists the means and standard deviations (SD) of all belief scores. The skewness of each belief score is as follows: -0.045 for religiosity, +0.269 for political leaning, +0.645 for trust in public institutions, and - 1.192 for vaccine hesitancy. More participants with increased feelings of vaccine hesitancy were represented in the study. Thus, the data was transformed into a normal distribution using the following equation:
Y (transformed vaccine hesitancy score) = SQRT (40 – vaccine hesitancy score)
Different transformations were tested to obtain a data spread that most resembled a normal distribution. The square root transformation reduced skewness to a greater extent than cubed or inverse transformations, because vaccine hesitancy scores that utilized the square root transformation had a more pronounced normal distribution compared to the other transformations. This transformed data was used for statistical testing. The transformed vaccine hesitancy score distribution is seen in Figure 2.
|
Belief Score |
Min |
Max |
Mean |
SD |
|
Religiosity |
||||
|
6 |
30 |
17.55 |
6.22 |
|
|
Political Beliefs |
||||
|
6 |
24 |
14.18 |
4.47 |
|
|
Trust in Public Institutions |
||||
|
8 |
26 |
15.58 |
3.72 |
|
|
Vaccine Hesitancy |
||||
|
16 |
40 |
33.03 |
5.50 |
|
Table 2. Means and standard deviations (SD) of belief scores.
Of all belief scores, vaccine hesitancy had the highest mean relative to its score range. This implies that more participants with increased feelings of vaccine hesitancy were represented in the study
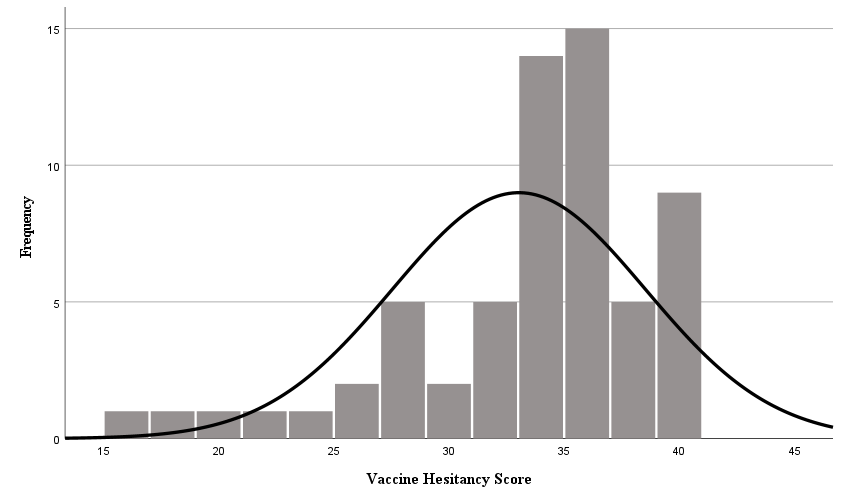
Figure 1. Distribution of Original Vaccine Hesitancy Scores. This distribution exhibits a right-ward skew, supporting the idea that more participants with increased feelings of vaccine hesitancy were represented in the study.
.png)
Figure 2. Distribution of Transformed Vaccine Hesitancy Scores. This new distribution exhibits a stronger normal distribution than the original distribution. The transformed data was utilized in all analyses.
Demographics & Bivariate Analysis on Belief Scores
The frequencies and P-values of all demographic variables and the belief scores are listed in Appendix 6. For brevity and clarity, we report the statistically significant findings in this paper. 45 participants (71.4%) identified as female, and 17 (27.0%) as male. 1 (1.6%) selected a gender identity of “other” . Because there was only 1 participant who did not identify as either male or female, and their response patterns were unusual, this participant’s responses were removed. We found that sex had no relationship with any of the belief scores.
The average age of participants was 32.0±10.8 years. The median age was 28.5 years. The youngest participant was 19 and the oldest was 71. Age was associated with trust in public institutions and vaccine hesitancy: As one aged, the less hesitant one becomes. 50 participants (80.6%) identified as Asian, 6 (9.7%) as white or Caucasian, 2 (3.2%) as Middle Eastern, 2 (3.2%) as mixed race, and 1 (1.6%) identified as Black or African American. 1 participant (1.6%) selected “other,” but did not specify a racial identity. Asian race was marginally associated with trust in public institutions. 32 participants (51.6%) attained a graduate or doctoral degree, 24 (38.7%) had a bachelor’s degree, 4 (6.5%) had some post-secondary education but no degree, 1 (1.6%) had a high school diploma or equivalent, and one (1.6%) had an associate degree. Education was associated with trust in public institutions and vaccine hesitancy; with a higher education level, there is less hesitancy.
Participants reported their combined household income before taxes in 2021. The average income was $121,383.87. The minimum income reported was $0 and the maximum income was $1,500,000. In examining the distribution, income was left skewed by +6.28, with more participants reporting lower incomes. Two data points with an income of $0 and one data point with an income of $1,500,000 were removed from the transformed dataset, because they were strong outliers and worsened the data skewness.
32 participants (50.8%) were employed or selfemployed, 7 (11.1%) were not employed and not looking for work, 4 (6.3%) were not employed and were currently looking for work, 2 (3.2%) were retired, 17 (27%) were students, and 1 (1.6%) was unable to work. Employment status was associated with trust in public institutions and vaccine hesitancy. 32 participants (51.6%) were married and 25 (40.3%) were single and never married. 3 participants (4.8%) were in a relationship and not married, 2 (3.2%) were divorced. Marital status was significantly associated with vaccine hesitancy, with married participants more hesitant. 20 participants (32.3%) reported having children under the age of 18 in their household while 42 participants (67.7%) did not. 49 participants (79.0%) identified as Sunni, 6 (9.7%) were Shia, 4 (6.5%) were Sufi, and 3 (4.8%) did not associate with any sect of Islam. Religious sect was associated with vaccine hesitancy; Sunnis were less hesitant of vaccines than non-Sunnis.
35 participants (55.6%) received most of their healthcare information from a licensed healthcare professional, 18 (28.6%) obtained it online, 3 (4.8%) utilized print media, 1 (1.6%) utilized radio, and 1 (1.6%) utilized television. 5 (8.1%) reported they used “other” sources. They received most information from scholarly sources, like peer reviewed journals, or clinical resources, like UpToDate.
61 participants (96.8%) received at least one dose of the COVID-19 vaccine, while 2 (3.2%) did not. Participants indicated their most important factor in receiving a vaccine. 23 (36.5%) were more willing if a vaccine had no safety issues. 8 (12.7%) were more willing if a vaccine did not cause potential allergies. 6 (9.5%) if a vaccine was free or low cost. 4 (6.3%) were more willing if a vaccine had no potential for causing autism or any other illness. 4 (6.3%) if vaccines had no pork-based ingredients. 4 (6.3%) were more willing because someone close to them had an illness. 2 (3.2%) were more willing because the people around them were receiving vaccines. Of the 12 participants (19%) who selected “other” as their most important factor for receiving a vaccine, 4 were more willing if the vaccine “actually prevented the disease,” 3 if there was proven scientific research and evidence for a vaccine, 2 if a vaccine had no side effects and 2 if they knew a vaccine could protect other people. 1 participant reported there was not one factor but rather many factors that affected their decision, and one participant reported they would get any vaccine recommended by their healthcare provider.
Additionally, participants reported on their most important reason for avoiding a vaccine. 15 participants (23.8%) were less likely to attain a vaccine if it had other safety issues not listed in the survey. 15 (23.8%) were less likely if they knew a vaccine was less efficacious, 8 (12.7%) if a vaccine had a potential for causing autism or any other illness. 7 (11.1%) selected “other” as an important factor for avoiding a vaccine. 7 (11.1%) were less likely if a vaccine caused potential allergies, 6 (9.5%) if a vaccine was expensive, 5 (7.9%) if a vaccine contained pork-based ingredients, and 4 (6.5%) who reported they had no reasons for avoiding a vaccine.
Correlation Analyses
Because age and income were continuous variables, correlation analyses were completed. We analyzed untransformed age and income values with each belief scores. Appendix 7 shows all findings for the parametric Pearson and non-parametric Spearman correlation. There was a significant positive Pearson correlation of age, household income, and religiosity score with the political beliefs score. Also, there was a significant positive Spearman correlation of age and religiosity score with the political beliefs score, income with religiosity score, and trust score with vaccine hesitancy. Because Spearman correlations are less sensitive to large outliers, there is a loss of statistical significance between income level with the religiosity score and political score. The strongest correlation is between the religiosity score and the political beliefs score (+.593).
Multiple Regression Analyses
Because none of the demographic variables were statistically significant on the religiosity and political beliefs scores, in the bivariate analysis, we did not complete multiple regression analyses on these scores. Appendix 8 and Appendix 9 show the multiple regression analyses for trust and vaccine hesitancy scores using two models. We discuss the statistically significant findings further.
Trust in Public Institutions
Model 1 compared the trust score with the statistically significant variables from the bivariate analysis. Model 2 compared the trust score with statistically significant variables and the other belief scores. In Model 1, participants older than 28.5 years were marginally more likely to have higher trust scores, controlling for race, education level, and employment status. In Model 2, participants with lower vaccine hesitancy scores were marginally more likely to have higher trust scores, controlling for the six other independent variables. Age ceased to be important in Model 2. 6.3% of the variability in trust was attributed to the four demographic variables in Model 1 (R2 = 0.063). 17.4% of the variability in trust was attributed to the four demographic variables plus the three other health belief scores in Model 2 (R2 = 0.174)
Vaccine Hesitancy
Model 1 tested the hesitancy score with the statistically significant variables from the bivariate analysis. Model 2 tested the trust score with the statistically significant variables and the other belief scores. According to Model 1 and Model 2, participants with a graduate or a doctorate degree were more likely to have higher hesitancy scores. This finding contradicts that of the T-test bivariate analyses. Moreover, Model 2 showed that participants with higher trust scores were marginally more likely to have lower vaccine hesitancy scores, with education remaining significant, controlling for all other variables. 10.2% of the variability in vaccine hesitancy was attributed to the five demographic variables in Model 1 (R2 = 0.102). 17.9% of the variability in vaccine hesitancy was attributed to the five demographic variables plus the three other health belief scores in Model 2 (R2 = 0.179). Lastly, there was no association between the vaccine hesitancy score and whether a participant received at least one dose of the COVID-19 vaccine.
Psychometric Testing
Since this study relies heavily on responses obtained from an online survey, we completed internal validity testing. The McDonald’s omega total for each belief score is as follows: religiosity = 0.893, political beliefs = 0.466, vaccine hesitancy = 0.864, trust in public institutions = 0.733. Internal validity testing was also completed using Cronbach alpha, which revealed the following scores: religiosity = 0.893, political beliefs = 0.600, vaccine hesitancy = 0.865, trust in public institutions = 0.792. Thus, the calculated belief scores on religiosity, vaccine hesitancy, and trust in public institutions reflected the most internal consistency. The low McDonald’s omega and Cronbach’s alpha for the political beliefs score may be due to participants interpreting questions differently or holding contradictory political and social attitudes. After all, individuals may not regard every aspect of a sociopolitical ideology with the same manner. There is diversity within individuals’ political beliefs.
Discussion
The goals of this study were to determine the factors that influenced vaccine hesitancy among Muslim-Americans and give healthcare providers a clear picture on how to address vaccine hesitancy with their Muslim patients, by learning about its prevalence and the socioeconomic factors that contribute to it. We hypothesized that vaccine hesitancy in Muslim-Americans follows anti-vaccination trends within the United States.
Demographic Factors
As age increased, vaccine hesitancy decreased, as confirmed by some studies [19, 28, 34, 35, 36] and contradicted by others [31, 32, 33]. More educated participants were less vaccine hesitant, which was supported by the multiple regression analysis. Similar relationships were found in some studies [3, 28, 35, 36] but contradicted in others [37]. Employed participants were less vaccine hesitant, which aligned with some previous research [28, 29] and not in others [30]. Furthermore, previous studies have reported that unmarried participants were more vaccine hesitant [28, 29, 36] which contradicts the findings of this study and others [31]. Lastly, participants who identified as Sunni were less vaccine hesitant than those who were nonSunni. No other study was found to have discussed hesitancy trends among Muslim sects, so this study was the first of its kind to determine statistically significant differences in vaccine acceptance between Sunnis and non-Sunnis. Ideally, more research will be conducted in the future to further elucidate the connection between sect and hesitancy. Only 9.7% of the sample represented Shias, whereas it’s estimated that 15%-20% of MuslimAmericans are Shia [57]. So, the differences in vaccine hesitancy compared to Sunnis is more of a speculative finding than one that is a proven public health trend.
Belief Scores
Religiosity
Income had a positive correlation with religious beliefs. There is no recent data on the connection between high income and stronger religious adherence compared with the findings of this study. In the last Religious Landscape Survey by the Pew Research Center from 2014, participants with higher incomes were less likely to attend religious services, have strongly associated beliefs in their faith or even align themselves with a particular religion [43]. So, while the findings of this study do not correspond with general trends between socioeconomic status and the extent of religious belief, any relationship between the two among Muslim-Americans is speculative. We do not have a strong theoretical framework on how income influences religiosity and vice versa. Additionally, participants with stronger religious beliefs favored more right leaning political, economic, and social ideologies. This aligns with general trends, like Americans with stronger religious leanings tend to follow conservative civic ideologies [44]. Because MuslimAmericans express and experience their religion in different ways, depending on sect and cultural background, it is difficult to determine what factors influence the extent of religiosity on other factors. While religiosity did not have a statistically significant relationship with trust in public institutions, a similar study on Muslim-Norwegians showed that the degree of religiosity worsened trust in the government and media [54].
Political Beliefs
Older age and higher income correlated with more conservative ideology in this study. While adults tend to have stable political beliefs over time, those who transition in their beliefs as they age are more likely to go from left leaning to right leaning [44].
Trust in Public Institutions
Participants were less likely to accept vaccines if they perceived that the institutions associated with them were not trustworthy or did not have the best interests of the public. The multiple regression analysis and other studies supported this [5, 7, 21, 26, 27, 44]. This finding was not surprising, as there are a multitude of factors that influence how Muslim-Americans perceive vaccines and the healthcare industry. These include but are not limited to socioeconomic barriers of healthcare access, systemic discrimination, Islamophobia and culturally uninformed health services [47].
For example, Muslim-Americans felt that the government limited COVID-19 relief to their communities and nonprofit organizations because of racist policies. These feelings of discrimination by the government aligned with a lack of trust in institutions. Even so, leaders from Muslim non-profit organizations were more likely to distrust the state government if they resided in a state with a strong Republican influence [51]. This aligns with other opinion polls, where Muslim-Americans expressed more trust in President Joe Biden and expressed low approval ratings for President Donald Trump compared to other religious groups [54]. Moreover, there are historical barriers to developing trust. For example, pregnant Arab women had worse birth outcomes after September 11, 2001 (9/11), due to the increased stigma around Muslims at this time [50]. The Patriot Act promoted intrusive surveillance of Muslim-American communities, which further isolated them and created an environment of paranoia. Three Muslim charities were labelled as terrorist organizations and eventually shut down [51]. In studies both in the U.S. and abroad, discriminatory socioeconomic and political policies create poor health outcomes for Muslims [47]
Unusual Findings
One association contradicted itself. Increased trust in public institutions and more education was associated with less vaccine hesitancy, but more education was not associated with higher trust scores. In an ideal scenario, more education would lead to more trust in public institutions and less vaccine hesitancy. The transformed vaccine hesitancy score data may have created this inconsistency. There was a positive association between trust in public institutions and more education with the untransformed data; however, the association became negative when untransformed vaccine hesitancy scores were analyzed with trust scores and education level. An explanation for this effect modification may originate in healthism, which refers to the “beliefs, behavior and expectations of the articulate, health-aware and information-rich middle-classes” [51]. Supporters of healthism may favor holistic, natural remedies over those of conventional medicine. They may view modern technology, especially that of vaccines, as unnatural and introducing unnecessary risks. Healthism is underpinned by a deep distrust of public institutions in favor of alternatives. Supporters usually have a plethora of unproven health information and research to refute conventional medical research. In this situation, it is the overabundance of false information that creates vaccine hesitancy, not the lack of well-documented evidence supporting vaccination.
Considerations, Limitations & Strengths
Online surveys with convenience sampling allow researchers to cast a wide net to attain participants with very little effort for recruitment. However, they pose problems with information validation. If a participant had at least one response that was an extreme outlier (± 3 standard deviations from the mean) or showed abnormal reporting patterns, all their responses were removed from the data analyses. This explains why only 62 participants were included in the final analysis, despite 65 participants meeting the inclusion criteria. Moreover, participants were asked about their opinions on vaccines for themselves, not for others, so there may be differences between how a person views vaccines for themselves or for someone else
Additionally, the survey was not distributed as widely as intended. Twenty-five Facebook groups were selected for distribution; however, only 10 disseminated the survey and they were dominated by South Asian and Sunni Muslims. To put this in context, only 1.6% of survey participants identified as Black or African American, but they make up 20% of Muslim population in America [45]. Also, the sample size was smaller than similar studies on vaccine hesitancy. However, the calculated minimum sample size for this study was 43, so the acquired 62 responses was higher than the smallest necessary sample. There may have been a more representative sample if Facebook advertisements were utilized, but this would have introduced new limitations, like increased study costs and high rates of survey attrition [46]. Unfortunately, Qualtrics did not provide completion data for this study’s survey, so an adequate comparison cannot be made.
Even so, there may be sampling bias. The lead author of this study is a South Asian Sunni woman in the medical field, who shared the survey in personal and academic circles. Thus, educated individuals with the means of accessing reliable health information resources, primary care physicians and healthcare services were overrepresented. Muslim-Americans practice in diverse ways. We inquired about halal vaccine ingredients, but this question may be interpreted in differing ways, depending on one’s sect, cultural background, and religiosity. Also, there is a social desirability bias for this study’s questionnaire. There is a possibility that participants implicitly overreported positive belief scores, like the extent of their religiosity. These discrepancies impacted the findings of this survey because there are statistically significant associations between education level and trust in public institutions with vaccine hesitancy
Lastly, there was a possibility that the multiple regression underestimated the effects of racial identity on vaccine hesitancy. Participants volunteered to share their opinions, so there may be recall bias, a Hawthorne effect, or incorrect recollections. There are numerous unmeasured confounding factors, like language barriers, previous experience with the American healthcare system and immigration background, which can influence belief scores. Unfortunately, it is difficult to quantify these factors into objective findings since they are subjective opinions.
To offset these limitations, the study had several analytical strengths. First, skewed variables were transformed into a normal distribution. Second, while the independent samples T-tests compared the means of the belief scores, the multiple regressions reduced the effect of confounding variables. The multiple regression models compared demographic and confounding variables. Lastly, internal validity testing strengthens analyses on religiosity, vaccine hesitancy, and trust belief scores. A proposed future study would aim to improve the diversity of the sample and the sample size.
Recommendations
Overall, public health scientists must have compassion and empathy when engaging the public on vaccination. Healthcare is a deeply personal choice that reflects one’s background, personal history, and beliefs. We show that distrust in public institutions increases vaccine hesitancy.
Thus, there must be transparency at all levels of public health infrastructure [47]. Government agencies can dispel misinformation about vaccines and communicable diseases through campaigns and advocacy [48]. Healthcare providers should utilize accessible language when educating their Muslim patients on the risks and benefits of vaccination. This can include incorporating brochures or translation services [47]. Also, by understanding vaccine hesitancy factors for each patient, clinicians can address individual concerns and personalize the healthcare experience [48].
We show that there are differences in vaccine acceptance between two major Islamic sects. While our sample size is small, there is so little information on specific vaccine hesitancy patterns among Muslim-American. This data is the first step in extrapolating Muslim-American healthcare patterns among different sects and in-groups.
While public health research focuses on determining broad healthcare trends in distinct groups, we believe our study is best suited as a primer for further questioning [53]. We aim for our study to also highlight pitfalls in recruiting participants online, so similar studies in the future can avoid our mistakes and obtain a more representative sample of Muslim-Americans. Moreover, the discrepancy in vaccine hesitancy between Sunnis and Shias, while a weak relationship, is an interesting speculation. Are Shias truly more vaccine hesitant or is this explained by their underrepresentation in the study? We hope our findings generate more interest in further studying if and to what extent Shia Muslim-Americans are vaccine hesitant. Even though our findings are preliminary, it highlights how a portion of the population can contain much diversity within itself. Clinicians should aim for proactive discussions with their Shia patients, as they should with all of their Muslim patients, by addressing concerns with vaccination early, dispelling misunderstandings, and reaffirming patients’ decision to vaccinate [47].
Finally, we recommend the use of culturally appropriate community-level outreach [49]. For example, public health outreach led by women would be more acceptable to female Muslim-Americans [48]. Also, since Islam has a diverse cultural tradition, mainstays of Muslim belief across all sects should be emphasized when developing advocacy strategies. For example, HPV can be transmitted by non-sexual contact, so an HPV vaccine can be beneficial for monogamous or celibate young patients [48]. This is a better approach than simply telling MuslimAmerican patients how HPV causes cervical and anal cancers [47]. Overall, we recommend against overly moralizing vaccines as it can alienate patients and cause further hesitancy. While it’s easy for healthcare workers to express frustration at those who harbor anti-vaccination sentiments, it’s important to remember that all people are pulled by their own biases and conflicts of interest. Thus, it is necessary to have a sense of optimism and remain proactive in developing people’s trust in vaccines.
Acknowledgements
Funding
The authors, individuals who assisted with the study, and study participants did not receive compensation for their involvement. No external funding or grants were utilized in the creation, distribution, and publication of this study.
Data Availability
All study data available on request from authors.
Conflicts of Interest
None declared.
Abbreviations
CDC: Centers for Disease Control and Prevention
U.S.: United States of America
HPV: Human Papilloma Virus
1. Morales DX, Paat YF. Hesitancy or Resistance? Differential Changes in COVID-19 Vaccination Intention Between Black and White Americans. J Racial & Ethnic Health Disp. 2024; 11: 23–35. doi:10.1007/s40615-022-01494-1.
2. Hossain MB, Alam MZ, Islam MS, Sultan S.; Faysal MM.; Rima S, et al. COVID-19 vaccine hesitancy among the adult population in Bangladesh: A nationwide cross-sectional survey. PloS One. 2021; 16: e0260821. doi:10.1371/journal.pone.0260821.
3. Sallam M, Dababseh D, Eid H, Al-Mahzoum K, AlHaidar A, Taim D, et al. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines, 2021; 9: 42. doi: 10.3390/vaccines9010042.
4. Hearld KR, Budhwani H. Human papillomavirus (HPV) and influenza vaccine behavior among Muslim women in the United States. Health Care for Women Intl. 2020; 41: 532–542. doi: 10.1080/07399332.2019.1623797.
5. Gidengil C, Chen C, Parker AM, Nowak S, Matthews L. Beliefs around childhood vaccines in the United States: A systematic review. Vaccine. 2019; 37: 6793– 6802. doi: 10.1016/j.vaccine.2019.08.068.
6. Johnson DK, Mello EJ, Walker TD, Hood SJ, Jensen JL, Poole BD. Combating Vaccine Hesitancy with Vaccine-Preventable Disease Familiarization: An Interview and Curriculum Intervention for College Students. Vaccines. 2019; 7: 39.
7. Justwan F, Baumgaertner B, Carlisle JE, Carson E, Kizer J. The effect of trust and proximity on vaccine propensity. PloS One. 2019; 14: e0220658.
8. Kempe A, Saville AW, Albertin C, Zimet G, Breck A, Helmkamp L, et al. Parental Hesitancy About Routine Childhood and Influenza Vaccinations: A National Survey. Pediatrics. 2020; 146: e20193852.
9. Alqahtani YA, Almutairi KH, Alqahtani YM, Almutlaq AH, Asiri AA. Prevalence and Determinants of Vaccine Hesitancy in Aseer Region, Saudi Arabia. Sultan Qaboos Univ Med J. 2021; 21: 532–538.
10. Alsubaie SS, Gosadi IM, Alsaadi BM, Albacker NB, Bawazir MA, Bin-Daud N, et al. Vaccine hesitancy among Saudi parents and its determinants: Result from the WHO SAGE working group on vaccine hesitancy survey tool. Saudi Med J. 2019; 1242–1250. doi: 10.15537/smj.2019.12.24653.
11. Kalok A, Loh S, Chew KT, Abdul Aziz NH, Shah SA, Ahmad S, et al. Vaccine hesitancy towards childhood immunisation amongst urban pregnant mothers in Malaysia. Vaccine. 2020; 38: 2183–2189.
12. Mohd Azizi FS, Kew Y, Moy FM. Vaccine hesitancy among parents in a multi-ethnic country, Malaysia. Vaccine. 2017; 35: 2955–2961. doi: 10.1016/j. vaccine.2017.04.010.
13. Martinez-Bravo M, Stegmann A. In vaccines we trust? the effects of the CIA’s Vaccine Ruse on immunization in Pakistan. JEEA. 2021; 20: 150–186.
14. Mohd Azizi FS, Kew Y, Moy FM. Vaccine hesitancy among parents in a multi-ethnic country, Malaysia. Vaccine. 2017; 35: 2955–2961. doi: 10.1016/j. vaccine.2017.04.010.
15. Martinez-Bravo M, Stegmann A. In vaccines we trust? the effects of the CIA’s Vaccine Ruse on immunization in Pakistan. JEEA. 2021; 20: 150–186.
16. Tefera YA, Wagner AL, Mekonen EB, Carlson BF, Boulton ML. Predictors and Barriers to Full Vaccination among Children in Ethiopia. Vaccines. 2018; 6: 22.
17. Memish ZA, Khan AA, Ebrahim S. Measles and the 2019 hajj: The risk of magnifying the global measles surge. BMJ. 2019; 26: 1–2.
18. Dyer O. Measles outbreak in Somali American community follows anti-vaccine talks. BMJ. 2017; 357. doi: 10.1136/bmj.j2378.
19. Murphy J, Vallières F, Bentall RP, Shevlin M, McBride O, Hartman TK, et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nature Comm. 2021; 12: 29.
20. Padmawati RS, Heywood A, Sitaresmi MN, Atthobari J, MacIntyre CR, Soenarto Y, et al. Religious and community leaders' acceptance of rotavirus vaccine introduction in Yogyakarta, Indonesia: a qualitative study. BMC Public Health. 2019; 19: 368.
21. Khan YH, Mallhi TH, Alotaibi NH, Alzarea AI, Alanazi AS, Tanveer N, et al. Threat of COVID-19 Vaccine Hesitancy in Pakistan: The Need for Measures to Neutralize Misleading Narratives. Amer J Trop Med & Hygiene. 2020; 103: 603–604.
22. French K. The Desperate Race for Halal Vaccines. Proto Magazine. 2019.
23. Eysenbach G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004; 6: e34. doi: 10.2196/jmir.6.3.e34
24. Lin C, Tu P, Beitsch LM. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines. 2020; 9: e0008961.
25. Pan F, Zhao H, Nicholas S, Maitland E, Liu R, Hou Q. Parents' Decisions to Vaccinate Children against COVID-19: A Scoping Review. Vaccines. 2021; 9: 1476.
26. Freeman D, Loe BS, Chadwick A, Vaccari C, Waite F, Rosebrock L, et al. COVID-19 vaccine hesitancy in the UK: the Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Abbrev Psych Med. 2020; 52: 1–15.
27. Lin Y, Hu Z, Zhao Q, Alias H, Danaee M, Wong LP. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Neglect Tropical Dis. 2020; 14: e0008961.
28. Dror AA, Eisenbach N, Taiber S, Morozov NG, Mizrachi M, Zigron A, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Euro J Epi. 2020; 35: 775–779.
29. Wang K, Wong EL, Ho KF, Cheung AW, Yau PS, Dong D.; et al. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines. 2021; 9: 62.
30. Palamenghi L, Barello S, Boccia S, Graffigna G. Mistrust in biomedical research and vaccine hesitancy: the forefront challenge in the battle against COVID-19 in Italy. Euro J Epi. 2020; 35: 785–788.
31. Kwok KO, Li KK, Wei WI, Tang A, Wong S, Lee SS. Editor's Choice: Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Intl J Nurs Stud. 2021; 114: 103854.
32. Detoc M, Bruel S, Frappe P, Tardy B, Botelho-Nevers E, Gagneux-Brunon A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine. 2020; 38: 7002–7006.
33. Fisher KA, Bloomstone SJ, Walder J, Crawford S, Fouayzi H, Mazor KM. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. A Int Med. 2020; 173: 964–973.
34. Al-Mohaithef M, Padhi BK. Determinants of COVID-19 Vaccine Accptance in Saudi Arabia: A Web-Based National Survey. J Multidis Healthcare. 2020; 13: 1657–1663.
35. Salali GD, Uysal MS. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psych Med. 2020; 52: 3750–3752.
36. Harapan H, Wagner AL, Yufika A, Winardi W. Anwar S, Gan AK, et al. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Frontiers in Public Health. 2020; 8: 381.
37. Wong LP. Alias H, Wong PF, Lee HY, AbuBakar S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Human Vacc & Immunotherap. 2020; 16: 2204–2214.
38. Kabir R, Mahmud I, Chowdhury M, Vinnakota D, Jahan SS, Siddika N, et al. COVID-19 Vaccination Intent and Willingness to Pay in Bangladesh: A CrossSectional Study. Vaccines. 2021; 9: 416.
39. Sabahelzain MM, Moukhyer M, Dubé E, Hardan A, van den Borne B, Bosma H. Towards a further understanding of measles vaccine hesitancy in Khartoum state, Sudan: A qualitative study. PloS one. 2019; 14: e0213882.
40. Kane SP. Sample Size Calculator. ClinCalc. 2024. Available from: https://clincalc.com/stats /samplesize .aspx
41. U.S. Citizen and Immigration Services. 10 Steps to Naturalization. 2022. Available from: https://www. uscis.gov/sites/default/files/document/brochures/M1051.pdf
42. Smith G. America’s Changing Religious Landscape. Pew Research. 2015. Available from: https://www .pewresearch.org/religion/2015/05/12/americaschanging-religious-landscape/
43. Levin J, Bradshaw M. Determinants of COVID-19 skepticism and SARS-CoV-2 vaccine hesitancy: findings from a national population survey of U.S. adults. BMC Public Health. 2022; 22: 1–8.
44. Peterson JC, Smith KB, Hibbing JR. Do People Really Become More Conservative as They Age?. J of Pol. 2020; 82: 600–611.
45. Mohamed B, Diamant J. Black Muslims account for a fifth of all U.S. Muslims, and about half are converts to Islam. Pew Research. 2019. Available from: https://www.pewresearch.org/fact-tank/2019/01/17/ black-muslims-account-for-a-fifth-of-all-u-smuslims-and-about-half-are-converts-to-islam/
46. Schneider D, Harknett K. What’s to Like? Facebook as a Tool for Survey Data Collection. Socio Methods & Res, 2022, 51, 108–140.
47. Hassan W, Kazmi SK, Tahir MJ, et al. Global acceptance and hesitancy of COVID-19 vaccination: A narrative review. Narra J. 2021,1: e57
48. Eguavoen A, Larson HJ, Chinye-Nwoko F, Ojeniyi T. Reducing COVID-19 vaccine hesitancy and improving vaccine uptake in Nigeria. J Global Health, 2023, 14: 1-5
49. Syadza S, Husnah H, Hajar S, Nauval I, Agung Pranata Atmaja RM. Balance nutrition and vaccination as efforts to prevent COVID-19 in the community: A cross-sectional study. Trends in Infection and Global Health, 2022, 2: 1-9.
50. Samari G. Islamophobia and Public Health in the United States. Am J Public Health. 2016;106 (11):1920-1925. doi:10.2105/AJPH.2016.303374
51. Kirbiš A. The Impact of Socioeconomic Status, Perceived Threat and Healthism on Vaccine Hesitancy. Sustainability. 2023, 15: 6107.
52. Noor Z., Wasif R., Siddiqui S., Khan S. Racialized minorities, trust, and crisis: Muslim-American nonprofits, their leadership and government relations during COVID-19. Nonprofit management & leadership. 2022, 32: 341–364. https://doi.org/ 10.1002/nml.21486
53. McDermott R. On the scientific study of small samples: Challenges confronting quantitative and qualitative methodologies. Leadership Quarterly, 2023, 34.
54. Ishaq, B., Bjertness, E., Østby, L., Johannessen, A., Schnell, T. Is the degree of religiosity related to community belonging and trust in society? A crosssectional study among Muslims in Norway. 2024, 10. doi:10.1016/j.ssaho.2024.101065
55. Coplen, K. Muslims Show More Trust in Public Officials’ Guidance on COVID-19. Institute for Social Policy and Understanding. 2022.
56. Mapping the Global Muslim Population. Pew Research. 2009. Available from: http://pewrsr.ch/13srCwM
57. U.S. Muslims Concerned About Their Place in Society, but Continue to Believe in the American Dream. Pew Research. 2017. Available from: https://www.pewresearch.org/religion/2017/07/26/fi ndings-from-pew-research-centers-2017-survey-ofus-muslims/