Chest Pain on Exertion: Atherosclerosis or Something Else?
Ahmad Morshed
MD, FACC, Attending, Interventional cardiology, Faculty, cardiovascular fellowship, Bassett medical center, Cooperstown, NY
Correspondence: Email: dr_morshed75@yahoo.comSingle coronary artery (SCA) is a rare congenital disease where a single coronary artery arises from the single coronary sinus. The majority of SCA cases are benign. This case presentation is about the management of 51-year- old gentleman with chest pain on exertion.
Chest Pain on Exertion: Atherosclerosis or Something Else?
Ahmad Morshed
MD, FACC, Attending, Interventional cardiology, Faculty, cardiovascular fellowship, Bassett medical center, Cooperstown, NY
Correspondence: Email: dr_morshed75@yahoo.com
Introduction
Single coronary artery (SCA) is a rare congenital anomaly in which there is an isolated coronary artery that arises from a single coronary ostium. Although the majority of patients with SCA are asymptomatic, some patients can present with life-threatening symptoms1 . Single coronary artery (SCA) is usually discovered incidentally and has an estimated incidence ranging between 0.024% and 0.066% among patients undergoing routine coronary artery catheterization2 . Single coronary artery (SCA) was first described by Lipton et al. in 19793 .
Case presentation:
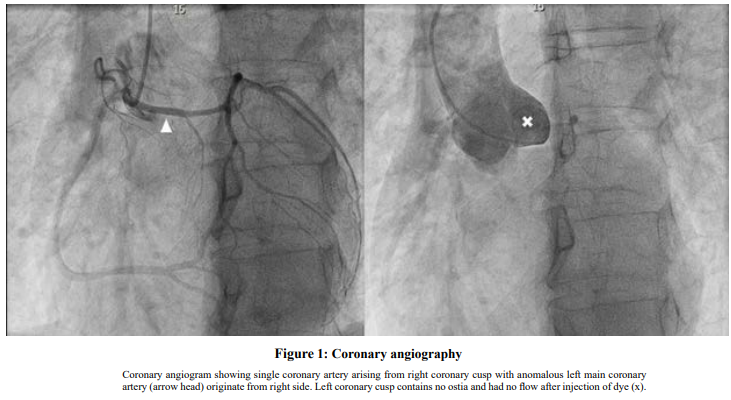
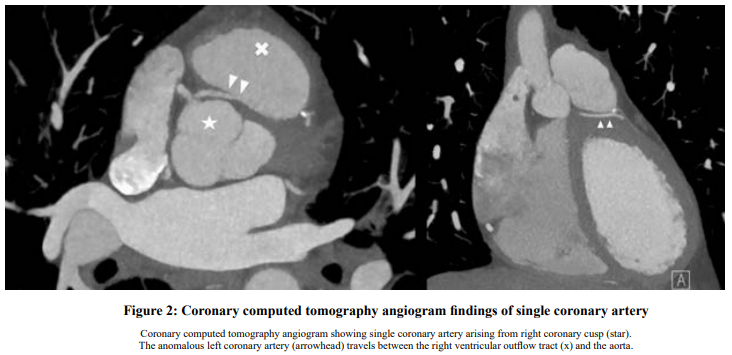
A 51-year-old gentleman presented to ED with chest pain and sob on exertion for 1 month. His past medical history is significant with chronic obstructive pulmonary disease. He is an active smoker with smoking 1-2 PPD for 30 years. On physical examination, his vital signs were normal and no significant abnormalities were noted in cardiovascular and other relevant systemic examinations. His electrocardiogram showed normal sinus rhythm with a right bundle branch block without new ST-T changes. High sensitivity troponin I was negative on arrival and in subsequent studies. An echocardiogram showed preserved left ventricular ejection fraction without regional wall motion abnormality. A nuclear stress test with regadenoson showed an abnormal study with borderline apical ischemia and a left ventricular ejection fraction of 49%. Coronary angiogram and supra valvular aortography showed left main (LM) and right coronary artery (RCA) arose from single ostium in right coronary sinus and LM trunk divided into LCX and LAD. Coronary CT angiogram confirmed an anomalous origin of the left coronary artery from the right coronary sinus as a common origin with the right coronary artery and left main trunk course is interarterial course between right ventricular outflow tract and aorta. There was mild atherosclerotic stenosis in the origin of left anterior descending artery. It was categorized as RII-S by modified Lipton’s classification. Low-dose aspirin, metoprolol and atorvastatin were started for atherosclerosis. The patient underwent unroofing procedure where the main pulmonary artery was separated from the aorta and the interventricular septal muscle was cut to elevate the left main artery till LM merges with epicardial artery. The procedure was done to decompress the LM. The patient tolerated the procedure well and was discharged to home. Follow-up echo showed slightly reduced LVEF (50%). Follow up visit in 3 months showed his chest pain and sob on exertion improved.
Discussion:
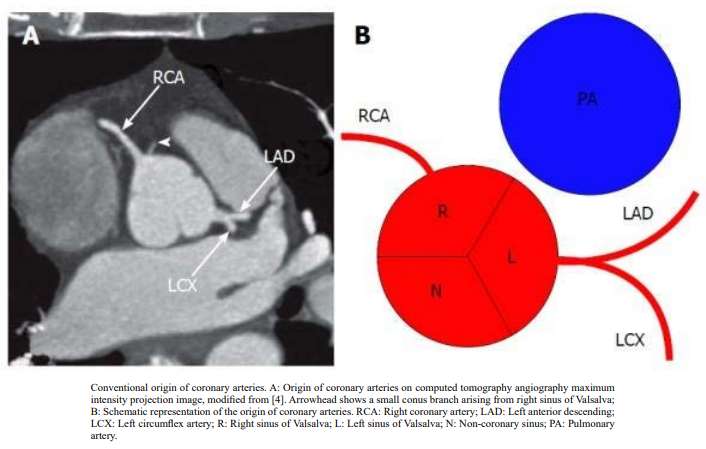
Normally, there are 2 main coronary arteries: the right coronary artery (RCA) and the left main artery (LM). LM divides into left circumflex artery (LCX) and left anterior descending (LAD). These 2 coronary arteries arise from 2 coronary sinuses (right and left coronary sinuses). Modified Lipton classification classifies single coronary artery into 3 groups3 . Group I is a true SCA with a normal course of a single coronary artery (LCA or RCA) that arises from a normal coronary sinus followed by the other vessel originating distally from the normal artery. Group II describes large SCAs arising from either the right or left coronary sinus, that then separate into two major coronary arteries, LCA and RCA, and subclassified the group by the path of the abnormal artery related to the aorta and PA into A (anterior to PA), B (between the aorta and PA), P (posterior to the aorta), S (intramuscularly through the septum, intraseptal), and C (combined type). Group III describes a patient with three arteries (RCA, LCA, and LAD) originating from a single coronary artery that arises from a single coronary sinus. Most of the SCA patients are asymptomatic. The diagnosis is made by either coronary angiography, CCTA, or cardiac magnetic resonance (CMR) imaging3,4 . IVUS can be used to check for slit-like origin or LM compression. SCA is less frequently associated with sudden cardiac death except interarterial (between pulmonary artery and aorta) or intraseptal course. The high-risk factors are slit-like/ fish-mouth-shaped orifices, acute angle takeoff, intramural course, and hypoplasia of the proximal coronary artery. Management is based on the course of the artery as well as management of symptoms. The American Heart Association recommended surgery with typical ischemic symptoms with a positive stress test as class 1 recommendation and Class IIa for those without symptoms5 . However, coronary artery bypass is not recommended for competitive flow with native vessel. The compression is mainly dynamic
Finally, there are some aspects of management that require more research. Although repair is mainly done in intraseptal or interarterial courses, data about the long-term outcome is not available and the role of stenting is not clear. There is not enough data about medical management.
1. Rashid Al Umairi1 and Maryam Al-khouri2 et al. Prevalence, Spectrum, and Outcomes of Single Coronary Artery Detected on Coronary Computed Tomography Angiography (CCTA).Volume 2019 |Article ID 2940148 | https://doi. org/10.1155/2019/2940148
2. W. Desmet, J. Vanhaecke, M. Vrolix et al., “Isolated single coronary artery: a review of 50 000 consecutive coronary angiographies,” European Heart Journal, vol. 13, no. 12, pp. 1637–1640, 1992.View at: Publisher Site | Google Scholar
3. Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L: Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979, 130:39-47. 10.1148/130.1.39
4. Young PM, Gerber TC, Williamson EE, Julsrud PR, Herfkens RJ. Cardiac imaging: Part 2, normal, variant, and anomalous configurations of the coronary vasculature. AJR Am J Roentgenol. 2011;197:816–826. [PubMed] [Google Scholar]
5. Stout KK, Daniels CJ, Aboulhosn JA, et al.: 2018 AHA/ ACC Guideline for the management of adults with congenital heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019, 139:e637- 97. 10.1161/CIR.0000000000000602