HYPERTENSION - COMPLIANCE ENSURES CONTROL: Challenges for Bangladeshi Americans in Compliance
Riffat E Tasnim Rahie ,Tahira Binte Hasan,Sadia Maisha,Md. Mamoon
Dhaka Medical College, Dhaka, Bangladesh
Armed Forces Medical College, Dhaka, Bangladesh
Sher-E-Bangla Medical College, Barisal, Bangladesh
Icahn School of Medicine, Queens Hospital Center, NY, USA
Corresponding Authors: Md. Mamoon
Correspondence: Attending, Icahn School of Medicine, Queens Hospital Center, NY, USAThe key factor in the management of hypertension is the patient's compliance with the treatment. There are some strategies a patient needs to follow all together to be compliant with the treatment of hypertension, and those are as follows: medication adherence, engaging in physical activity, adherence to the Dietary Approach to Stop Hypertension (DASH) diet, etc. We have performed an analysis to determine the patient's compliance with the treatment of hypertension based on the questionnaires filled out by the hypertensive patients visiting their doctor's office for follow-up. The subjects were of Bangladeshi descent and followed a particular dietary and lifestyle pattern. An intricate network of factors impacting compliance in HTN control was discovered through questionnaire analysis. The Morisky Medication Adherence Scale was used to assess compliance. Scoring according to the MMAS-4 scale revealed that a higher percentage of participants had medium to low adherence to the prescribed medication regimen, in contrast with a lower percentage of participants who had high adherence to the prescribed medication regimen. As the participants were of Bangladeshi descent and their diet is traditionally rich in red meat and fried food, this high prevalence of an unrestricted diet led to a higher percentage of participants having uncontrolled blood pressure. A higher percentage of patients who participated in more physical activity had blood pressure that was under control. On the other hand, we found out that for some participants, instead of having an active lifestyle, other factors such as non-adherence to medication and the DASH diet contributed to their poor control of blood pressure. In our study, we also discussed the importance of the patient's compliance with the treatment of hypertension and the strategies to be compliant with the treatment.
HYPERTENSION - COMPLIANCE ENSURES CONTROL: Challenges for Bangladeshi Americans in Compliance
Riffat E Tasnim Rahie ,Tahira Binte Hasan,Sadia Maisha,Md. Mamoon
Dhaka Medical College, Dhaka, Bangladesh
Armed Forces Medical College, Dhaka, Bangladesh
Sher-E-Bangla Medical College, Barisal, Bangladesh
Icahn School of Medicine, Queens Hospital Center, NY, USA
Corresponding Authors: Md. Mamoon
Correspondence: Attending, Icahn School of Medicine, Queens Hospital Center, NY, USA
Introduction
A significant issue in the treatment of hypertension has been patient compliance, or adherence, while we have been managing this disease process.[1] Numerous factors that the WHO has identified and that are present in nearly all patients with chronic diseases who have significant non-compliance rates lead to non-adherence to therapeutic regimens.[2] In hypertensive patients, non-compliance with pharmaceutical therapy varies between 45.2% (95% CI 34.4 to 56.1) and 63.35% (95% CI 38.78 to 87.91), while non-compliance with diet and physical activity is represented by 68.8% and 30.9%, respectively, for factors related to modifications to lifestyle.[2] According to scientific research, in order for patients to take their medications as prescribed and maintain dietary and physical activity improvements, it is necessary to use both pharmaceutical and non-pharmaceutical therapies to achieve an ideal SBP or DBP level.[2] As a result, they will see improvements in the management of hypertension, which will lead to a decrease in the burden of the disease and medical expenses.[2] The Dietary Approach to Stop Hypertension (DASH) diet is regarded as a preventative measure for blood pressure management with additional advantages for cardiac function as well as structure.[3] There was a considerably decreased incidence of hypertension when vigorous physical exercise or moderate exercise occurred more frequently and for longer periods of time.[4]
Materials and Method
A cross sectional study was performed based on a questionnaire, which was designed to highlight the impact of physical activity, dietary habits, and medication compliance on control of HTN. The questionnaire was filled out by hypertensive patients visiting the Doctor’s office for follow-up. The participants were Bangladeshi Americans who had a specific pattern of diet. The participants had a mean age of 55.4, among whom 52.9% were female and 47.1% were male. According to the questionnaire, the average BP of the participants was 139/89 measured with automated BP machine. The questionnaire was designed in a way that it revealed detailed information about dietary habits of participants. It also highlighted the physical activity level of the participants including frequency of it. Additionally, compliance to prescribed medication regimen was determined using Morisky Medication Adherence Scale (MMAS-4) and analysis was done accordingly.
Results
Detailed analysis of the questionnaire revealed a complex web of factors influencing compliance in HTN control. The complex web consists mainly of medication non-compliance, physical inactivity, and unrestricted diet.

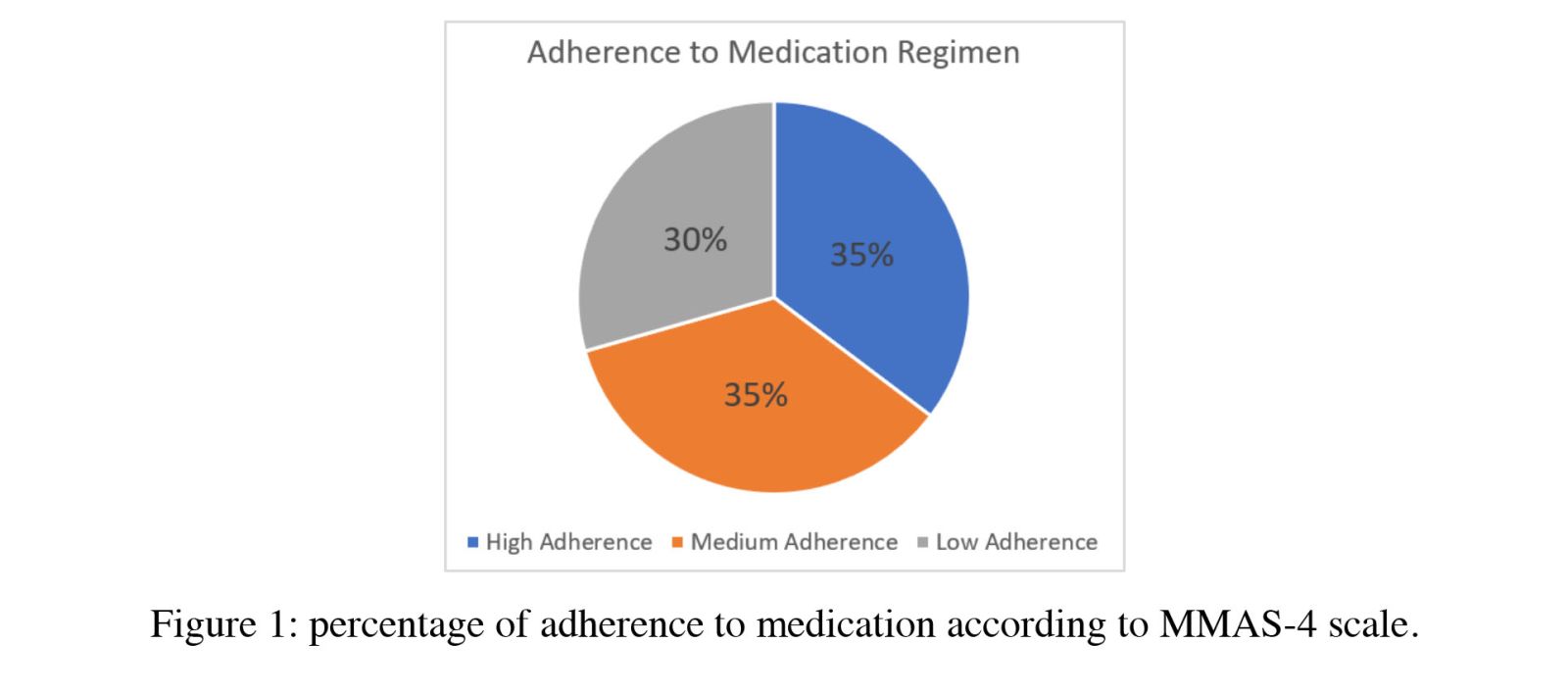
Scoring according to MMAS-4 scale revealed 35.29% participants had medium to low adherence to prescribed medication regimen in contrast with 29.4% participants who had high adherence. This percentage depicts that one of the vital contributors to uncontrolled BP is medication nonadherence and this nonadherence was prevalent among our Bangladeshi American cohort.
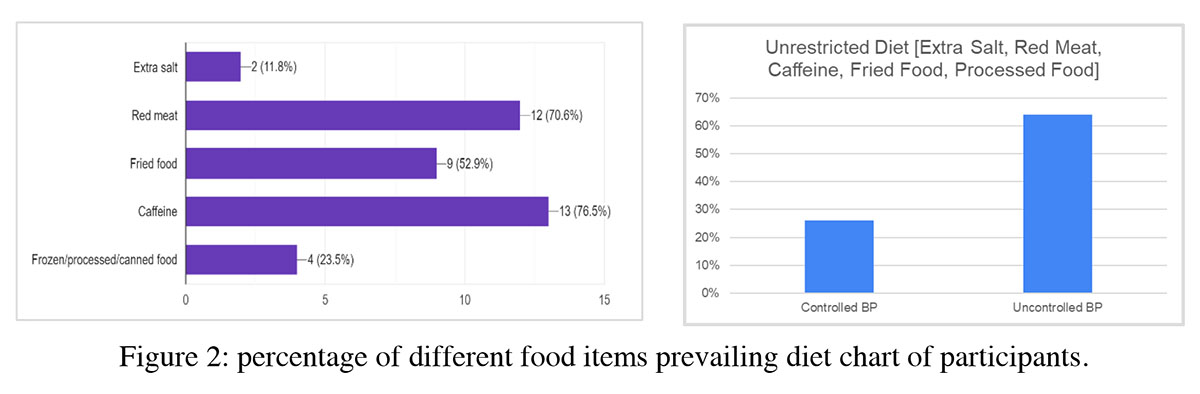
As the study was done in Bangladeshi American people and their diet is traditionally rich in red meat, fried food, spicy and oily food, this unrestricted dietary habit contributed to a greater extent to uncontrolled BP. The analysis shows that participants of our study reported high intake of red meat, fried food, and caffeine. This dietary habit led to the existence of uncontrolled BP in 62% of participants.
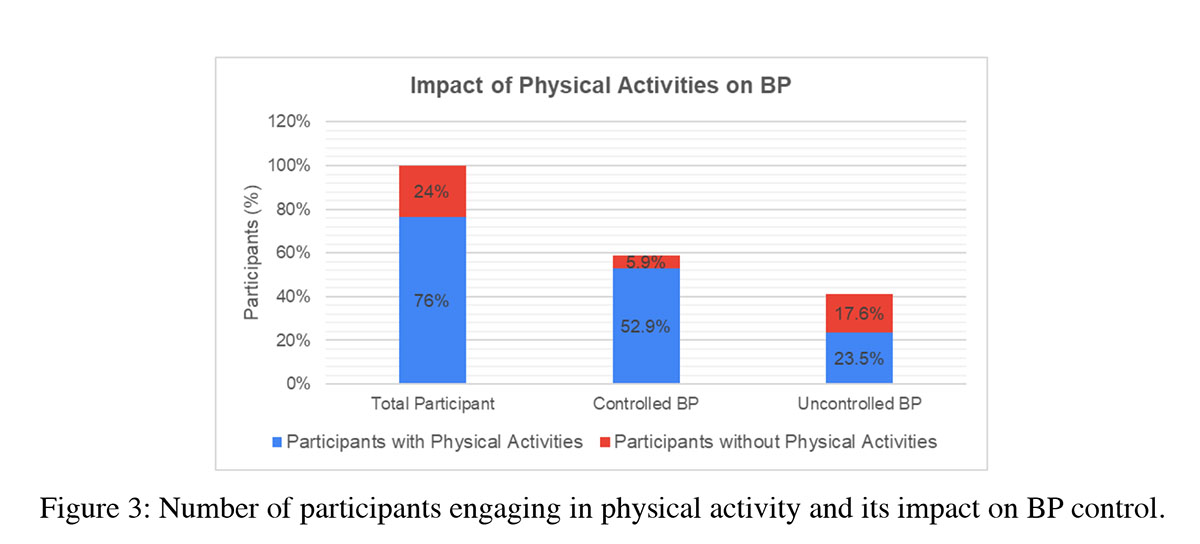
According to the above-mentioned graph 76% of participants reported engaging in physical activity but only 30.8% of them engaged in physical activity on a daily basis.
A well-controlled BP was documented in 58.8% of participants, among whom 52.9% were found to engage in physical activities. On the contrary, 41.1% had uncontrolled BP. Although 23.5% of them had an active lifestyle but other factors such as nonadherence to medication and DASH diet contributed to their poor control.
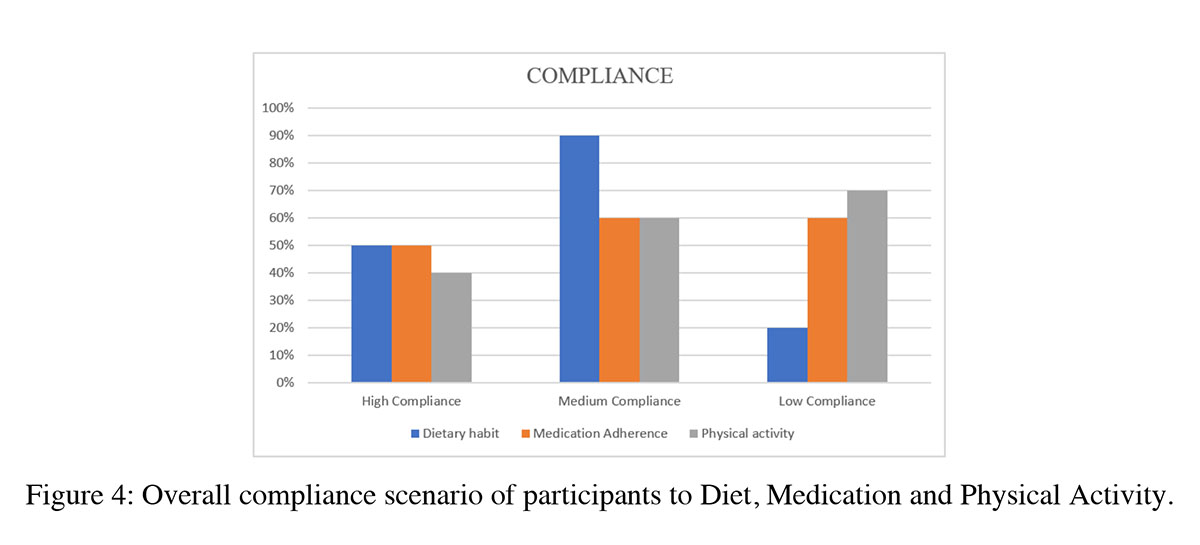
This graph below demonstrates the overall compliance of participants to DASH dietary habit, medication adherence, and physical activity.
Discussion
Hypertension is a chronic condition that affects many individuals worldwide, and controlling it is a major challenge in primary health care [6].
From our experimental study among the Bangladeshi population living in NY, we can see that the prevalence of hypertension is high. This is mainly because of diet and not having an active lifestyle. Traditionally, Bengali diet consists of red meat, high salt content, and oily fried food in comparison to Western population. This contributes to most people having the disease. Another significant cause is not understanding the importance of adherence to medication. A lot of the patients aren't willing to take or forget to take their daily dosage of anti-hypertensive when they are feeling well.
The guidelines from the American College of Cardiology (ACC)/American Heart Association (AHA) and the European Society of Hypertension (ESH)/European Society of Cardiology (ESC) recommend various nonpharmacological interventions for managing high blood pressure [6]. They are:
- Restricted intake of salt: Limiting the consumption of salt (sodium) can help lower blood pressure.
- Weight loss: Losing excess weight, particularly if overweight or obese, can have a significant impact on reducing blood pressure [6].
- Physical activity: Engaging in regular physical activity, particularly aerobic exercise (brisk walk, jogging, cycling, or swimming), is beneficial for preventing, treating, and controlling hypertension. Structured exercise programs are recommended, and the guidelines emphasize the importance of specifying the frequency, intensity, time, and type (FITT) of exercise regimens. [6]
- Dietary Approaches to Stop Hypertension (DASH) diet: The DASH diet emphasizes a high intake of fruits, vegetables, whole grains, fiber, low or free fat dairy product, legumes and nut intake and potassium, while minimizing fat, red and processed meat, sugar-sweetened beverages, and sodium consumption. [7] [8]. This diet has been shown to be effective in lowering blood pressure.
- High intake of fruit and vegetables: Fruits and vegetables are rich in essential nutrients, fiber, and antioxidants, which can contribute to the management of hypertension.
These interventions can be effective as standalone approaches or in combination with antihypertensive medications, depending on the individual's condition and healthcare provider's recommendations.
The following methods can be used to improve compliance to anti hypertensives in patients:
- Educational intervention to patient and the family members. [9.]
- Improve dosing schedule: use of pill boxes to organize daily medications, simplify the dosing regimen, hints to remind patient to take the medication like setting up alarm on the phone etc. [10].
- Clinic scheduling strategies: making follow up visits, shorter wait times, involvement of ancillary staffs like pharmacist, nursing staff, behavioral specialists [10].
- Improved communication between physician and patients [10].
Conclusion
This study was conducted on Bangladeshi Americans, who are mostly not adherents to the DASH diet because their traditional diets are heavy on fried foods and red meat. And so, despite having engagement in physical activity, the high prevalence of dietary freedom mostly contributed to the high rate of uncontrolled blood pressure among the participants. If we want to have an impact on blood pressure control, we must increase patient adherence to therapy. With the right strategy, many of the significant problems that affect compliance are capable of being resolved.[1] The relationship between diet and risk reduction is additionally strengthened by improved diet adherence.[5] Blood pressure levels were shown to be lower in people who engaged in high amounts of physical exercise and who had favorable views toward physical activity. Awareness about significance of compliance to DASH diet, medication regimen, and physical activity is the key to controlled BP in Bangladeshi Americans.
- Neutel, J. M., & Smith, D. H. (2003). Improving patient compliance: a major goal in the management of hypertension. Journal of clinical hypertension (Greenwich, Conn.), 5(2), 127–132. https://doi.org/10.1111/j.1524-6175.2003.00495.x
- Parra, D. I., Trapero Gimeno, I., Sánchez Rodríguez, J. M., Rodríguez Corredor, L. C., Hernández Vargas, J. A., López Romero, L. A., García López, F. J., Escudero-Gómez, C., Trujillo-Cáceres, S. J., Serrano-Gallardo, P., & Vera-Cala, L. M. (2020). Individual interventions to improve adherence to pharmaceutical treatment, diet and physical activity among adults with primary hypertension. A systematic review protocol. BMJ open, 10(12), e037920. https://doi.org/10.1136/bmjopen-2020-037920
- Yang, Y., Yu, D., Piao, W., Huang, K., & Zhao, L. (2022). Nutrient-Derived Beneficial for Blood Pressure Dietary Pattern Associated with Hypertension Prevention and Control: Based on China Nutrition and Health Surveillance 2015-2017. Nutrients, 14(15), 3108. https://doi.org/10.3390/nu14153108
- Zhou, L., Feng, W., Xiang, N., Cheng, Y., Ya, X., Wang, M., Wang, X., & Liu, Y. (2022). Association between physical activity dimensions and the risk of hypertension among middle and older adults: A cross-sectional study in China. Frontiers in public health, 10, 995755. https://doi.org/10.3389/fpubh.2022.995755
- Soltani, S., Arablou, T., Jayedi, A., & Salehi-Abargouei, A. (2020). Adherence to the dietary approaches to stop hypertension (DASH) diet in relation to all-cause and cause-specific mortality: a systematic review and dose-response meta-analysis of prospective cohort studies. Nutrition journal, 19(1), 37. https://doi.org/10.1186/s12937-020-00554-8
- Islam, F. M. A., Islam, M. A., Hosen, M. A., Lambert, E. A., Maddison, R., Lambert, G. W., & Thompson, B. R. (2023). Associations of physical activity levels, and attitudes towards physical activity with blood pressure among adults with high blood pressure in Bangladesh. PloS one, 18(2), e0280879. https://doi.org/10.1371/journal.pone.0280879
- Effectiveness of a multifactorial intervention, consisting of self-management of antihypertensive medication, self-measurement of blood pressure, hypocaloric and low sodium diet, and physical exercise, in patients with uncontrolled hypertension taking 2 or more antihypertensive drugs 10.1097/MD.0000000000019769
- Appel L.J., Moore T.J., Obarzanek E., Vollmer W.M., Svetkey L.P., Sacks F.M., Bray G.A., Vogt T.M., Cutler J.A., Windhauser M.M., et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997;336:1117–1124. doi: 10.1056/NEJM199704173361601.
- Fung T.T., Chiuve S.E., McCullough M.L., Rexrode K.M., Logroscino G., Hu F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008;168:713–720. doi: 10.1001/archinte.168.7.713.